Ovarian Cysts
NORMAL OVARIAN CYSTS
Physiological, follicular, or corpus luteal cysts are the normal cysts (fluid-filled sacs) with eggs that we have on our ovaries. They appear “simple” or fluid-filled on ultrasound. They come and go.
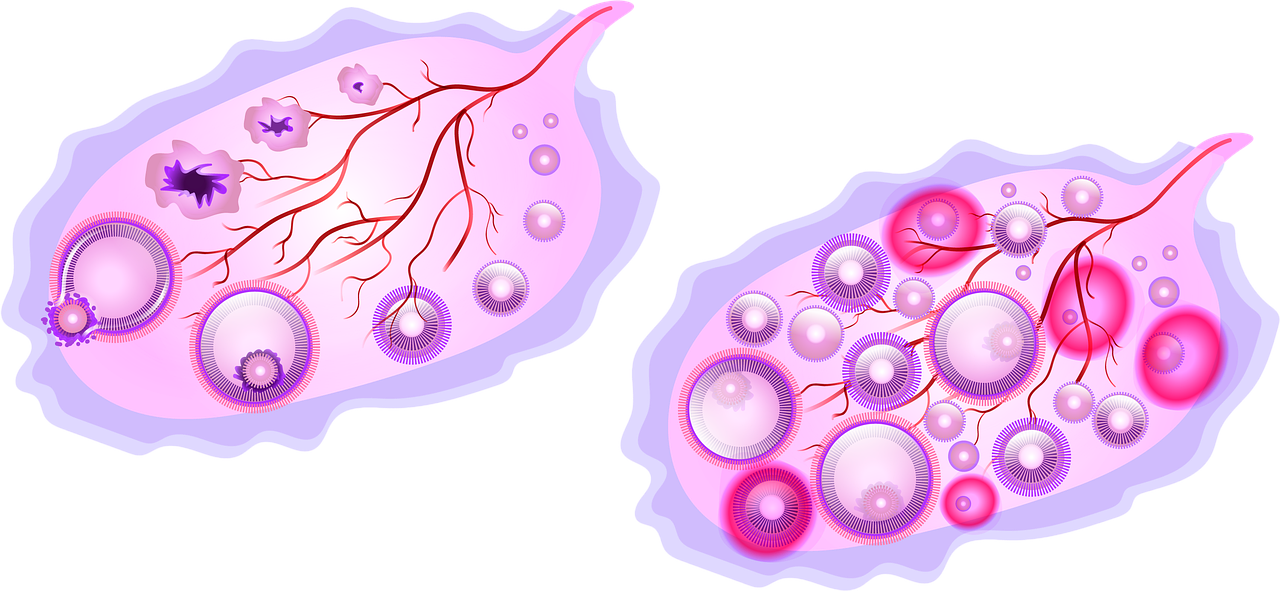
Every month, 1 egg ruptures or pops out from a growing cyst. Normally, this happens without any problems and we don’t notice it in the 400 times this can happen in our lifetime. Ovulation usually occurs mid-cycle. A period happens 2 weeks later if not pregnant.
We have lots of eggs in cysts, which is why it can be normal to see an ovarian cyst on pelvic ultrasound from time to time that later disappears. The best time to do a pelvic ultrasound to avoid seeing normal asymptomatic cysts, is right after your period.
Some women feel ovulation and it is called “mittelschmertz” or “little pain in the night.” Rarely, the cyst ruptures and releases the egg and it hurts a lot, by causing a hemorrhagic cyst where it bleeds into itself. A painful cyst rupture can also be triggered by intercourse mid-cycle if you’re about to ovulate. (Avoid mid-cycle sex to prevent rupturing an ovulation cyst and also if trying to avoid pregnancy. The egg lives for 12-24 hours.) This can cause a couple weeks of intense pain from the pressure of the clotted blood. A repeat ultrasound will show that the “complex” cyst has disappeared in 4-6 weeks. One can prevent recurrent painful ruptured cysts by taking birth control pills, patches, ring, progestin injection (these all suppress ovulation and emulate pregnancy when there is no need to ovulate). It would be rare for such painful ruptured ovarian cysts to keep recurring even though the experience can be so painful and may have necessitated an ER visit.
For more info about NORMAL kinds of ovarian cysts, see Youngwomenshealth.org
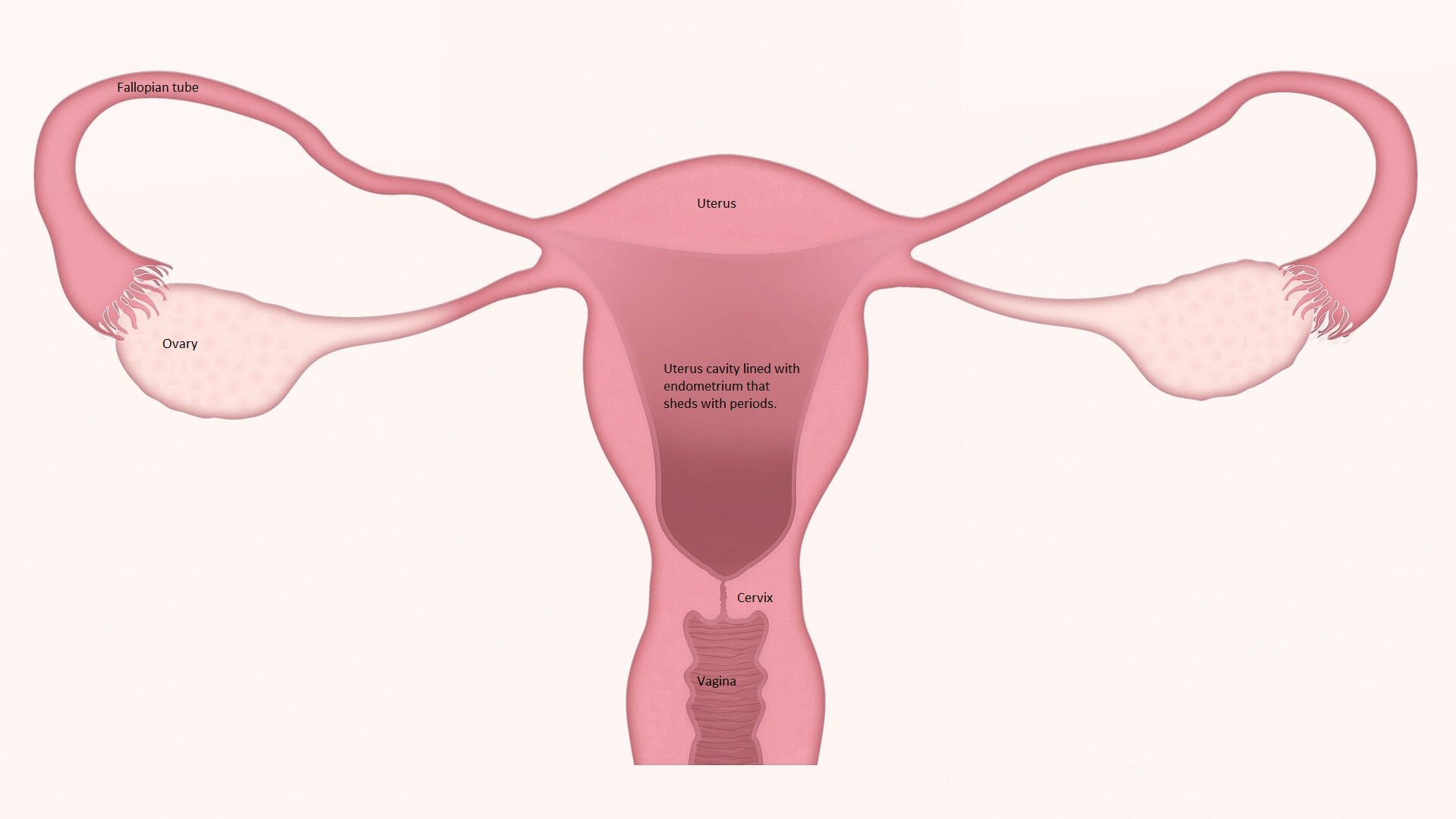
In Polycystic Ovarian Syndrome (PCOS), the cysts are still normal but laid out in a pearl necklace fashion around the edges of the ovary. The problem in this condition of missing periods, is that the eggs don’t get released. This is called Anovulation and that is why the period is skipped. Ovulation (egg release) causes a period 2 weeks later if there is no pregnancy. Dr. Kirkham spoke to Global News about PCOS.
ABNORMAL OVARIAN CYSTS
All cysts grow inside the ovary, like a balloon inside the outer ovarian balloon. Abnormal cysts (not the usual ones with eggs that we all have on our ovaries) can appear “complex” on ultrasound because they contain more than clear fluid.
Not all abnormal cysts are cancerous. Surgical removal of cysts (by shelling them out of the ovary = cystectomy, or removal of the ovary = oophorectomy) tells us what type of cyst they are exactly. Gynecologists try hard to preserve your fertility (ability to have babies) by taking out the cyst only when appropriate. Laparoscopy (keyhole) day surgery is used.
Cystadenomas: These can grow large and be filled with a mucous-like fluid. They are usually benign (not cancerous).
Dermoid cysts: Dermoid cysts are made of cells from other parts of the body such as hair, skin, teeth. They are the most common type of abnormal cysts but still, most are not cancerous. When small, they can be left alone. If they grow fast, are concerning for other types of cysts, are big enough to cause pain or pressure, or twist, the cyst only (leaving the ovary inside you) can be removed through laparoscopic (keyhole) day surgery.
Endometriomas: These are also called “chocolate cysts” because when we remove them during surgery, they look like melted chocolate contents. When both ovaries have endometriomas and they touch, they are called “kissing ovaries.” Endometriomas are related to endometriosis, which is a chronic painful period condition where the lining of your uterus grows outside the uterus in the pelvis. The pelvis is the space inside your abdomen that also contains your bowels, bladder, ovaries. This is why people with endometriosis often have pain or pressure symptoms with bowel movements, urination, periods, sex or nonmenstrual daily pain. Endometriomas can be treated with medicine or surgery depending on size and symptoms.
Low malignant potential or borderline cysts: These are rare and often diagnosed and cured after surgery. Close follow up is recommended.
Ovarian cancer: Cancer of the ovary is extremely rare for women under 40. Certain features of cysts from imaging can elevate risk of malignancy. Risks include family history, unhealthy lifestyle habits, postmenopausal status, endometriosis, and genes such as BRCA 1/2. Birth control pill use for 5-10 years, pregnancy, breastfeeding, and removal of fallopian tubes reduce risks of ovarian cancer.
OVARIAN TORSION
Torsion is a rare condition where a heavy ovarian cyst (usually a 5cm dermoid cyst) causes the ovary to twist. This is a gynecological emergency and the pain, nausea, +/or vomiting will usually make you go to the emergency room. Laparoscopy surgery is used to untwist the ovary and remove the cyst, which brings back the blood flow to the ovary.